|
University of Pittsburgh, School of Medicine, 931
Scaife Hall, Pittsburgh, PA 15261, USA
The structure and kinetics of the hematopoietic stem cell compartment
have long been the subject of considerable speculation. Based on
morphologic observations of normal and abnormal human marrow and
of a perturbed system in experimental animals, primarily the rabbit,
in 1938, Downey [1] concluded there was a stem cell capable of giving
rise to all hematopoietic tissue. He believed this cell in turn
gave rise to a lymphoid stem cell and to a myeloid stem cell. The
myeloid stem cell could give rise directly to erythroid, megakaryocytic
and monocytic cell lines and in turn produced a tertiary stem cell
which could generate neutrophils, eosinophils and basophils. With
the development of functional assays for clonal cell growth in vivo
and in vitro and through the use of chromosome marked clones this
suggested structure has proved to be correct in substance although
certain minor variations are indicated. Most definitive studies
of the structure of the stem cell compartment are in mice [2] but,
in general, the data generated in human diseases suggest that the
human stem cell structure is the same as that of the mouse. In Fig.
1, one current "best guess" is shown. There seems little doubt that
at least 3 concatenated precursor compartments exist for all myeloid
cells. Whether there are still more intermediate stages and whether
or not most cells forming colonies in vitro are stem cells (i.e.
capable of self-replication) remain open question. Studies from
Phillips Laboratory [2] using irradiation induced chromosomally
marked clones injected into W /WV mice have shown the presence of
an hematopoietic stem cell which is totipotent for all hematopoietic
cells, lymphoid as well as myeloid (THSC) and distinct from a cell
pluripotent for myeloid tissue (PMSC). This latter cell produces
spleen colonies in irradiated recipients and is, therefore, also
known as a colony forming unit cell (cru-S), but whether other classes
of cells will also produce spleen colonies is unknown. The structure
of the lymphoid compartment as derived from the THSC will not be
discussed. A cell which is restricted to the production of neutrophil-monocyte
colonies in vitro. colony forming unit -culture, (cru-C) has characteristics
distinguishing it from the CFU-S. Among a variety of differences
including a much higher percent in DNA synthesis [3], perhaps the
most convincing is the presence of normal CFU-C in the W /WV /mouse
in the face of very abnormal behaving CFU-S [4]. Cells apparently
restricted to production of erythroid (burst forming unit. BFU-E)
[5] megakaryocytic (CFU-meg) [6] and eosinophilic (CFU-Eos) [7]
are also demonstrable by in vitro analysis.
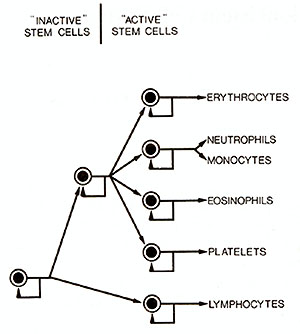
Fig. I. A model of the Hematopoietic stem cell system.
Three concatenated cell systems are presented. "Active'. refers
to the fact that a high percentage ofcells forming colonies in vitro
are in DNA synthesis while the more pluripotent spleen colony forming
cell compartment has few cells in DNA synthesis
At the present time, human diseases of the stem cell system appear
to involve either the THSC or the PMSC (CFU-S) compartment, although
specific defects in more committed compartments may possibly explain
diseases of a single cell line such as Diamond-Blackfan anemia or
certain forms ofcongenital neutropenia. However, no clonal markers
have been identified in these conditions. There is evidence that
the myeloid leukemias (ML) acute (A) and chronic (C) involve a wide
spectrum of hematopoietic tissue. In the case ofAML the most common
morphologic expression is by an increase in myeloblasts. However,
the cells often have some monocytic features as well and any of
the myeloid cell lines may appear as the predominant morphologic
expression in AML (Table 1). The very frequent myeloblast-monocyte
morphologic mix
Table I. Morphologic expressions of myeloid
leukemia
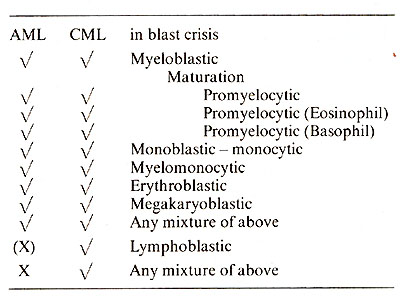
ture may reflect the immediate common origin of these cells. To
date there has been no means of separating individual precursors
for these cell lines in the in vitro clonal assays. When colonies
ofhuman or murine cells are grown in semi-solid media in the presence
of colony stimulating factor, mixed colonies of neutrophils and
monocytes occur [7]. Is AML one basic disease involving a pluripotent
myeloid stem cell or a series of diseases involving the specific
progenitors: such as, CFU-C or BFU-E, etc? Put another way, if these
are induced by an oncornavirus, what is the primary target cell?
There are anum ber of fairly simple clinical observations which
bear on this question. First of all, there is almost never a shifting
myeloid-lymphoid picture in AML and a mixed myeloid-lymphoid presentation
ofAML is not recognized. AML is defined arbitrarily in this paper
as excluding any patient in whom the Ph I chromosome is present
for I have observed an apparently mixed myeloid-lymphoid blastic
pattern in patients presenting with PhI positive acute leukemia.
Such patients are defined, again somewhat arbi1rarily, as presenting
in the blastic those of CML (see below). Thus, the THSC does not
appear to be involved in AML. However, a shifting morphologic expression
within myeloid cell lines does occur. Perhaps the most commonly
recorgnized shift is in the patient who presents with a predominantly
erythroblastic picture but proceeds to develop an increasing predominance
of myeloblasts or myelomonoblasts. Even when the predominant cell
is a myeloblast at the time of diagnosis. megaloblastic erythroid
precursors and abnormally small megakaryocytes are often present
if the marrow smear is searched with diligence. This suggests that
more than one myeloid cell line is involved in the AML process and
suggests that the target cell is the PMSC rather than the more differentiated
CFU-C systems. This is supported by chromosomal studies in which
rnarker chromosomes in the myeloblastic cells have also been found
in erythroid cells [8]. Clinical observations in CML suggest the
target cell may be the THSC. During the chronic phase, abnormalities
ofall of the myeloid cell series may be observed suggesting that
the leukemic clone is at least feeding through the PMSC. During
acute transformation, all of the morphologic spectrum seen in AML
may appear and, furthermore, a lymphoblastic or even a mixed lymphoblastic-AML
picture may develop [9]. The Philadelphia chromosome is found in
erythroid precursors, megakaryocytes, monocytes and eosinophils
as well as in neutrophil precursors [ 10]. Uniformity ofG-6 PD isozymes
in the myeloid series of patients whose non-hematopoietic cells
are heterozygous confirms the clonality of the disease and again
indicates involvement ofmore than one cell in the myeloid series
[II]. Furthermore, such heterozygotes may also have certain lymphocyte
populations homozygous for the isoenzymes, strongly suggesting that
the THSC is the target cell [ 12]. Polycythemia Rubra Vera (PRY)
and idiopathic myelofibrosis (IMF) are also diseases in which there
is clinical evidence for disturbance in cell production of all of
the myeloid cell systems. Analysis of G-6 PD isozyme data is compatible
with the concept that these diseases are also clonal diseases of
myeloid stem cells [II]. In paroxysmal nocturnal hemoglobinuria
there is evidence for abnormality ofneutrophils and platelets as
well as for red blood cells suggesting that this also might be a
disease of the pluripotent myeloid stem cell [ 13]. As yet. there
is little data which will allow one to make a guess as to whether
these diseases are at the level of the THSC or the PMSC. However.
the report of the development of acute lymphoblastic leukemia in
a patient with PRY [ 14] favors the THSC rather than the PMSC being
the affected cell. Still other diseases. such as aplastic anemia
and cyclic neutropenia are diseases which appear to involve myeloid
stem cells, although it seems unlikely that they are clonal. How
does a single stem cell take over the entire production of the myeloid
system? In most patients. chromosomal and isozyme data indicate
that all cell production is from the clone and in vivo evidence
for persistent growth of normal stem cells is lacking. Evidence
relative to the question of whether normal cells are still present
is discussed below. As a generality. when we observe a clone of
cells which is growing with seeming inappropriateness and eventually
leading to death we make a diagnosis of a malignant neoplasm. For
this reason most now consider PRY and IMF as well as AML and CML
to be malignan t neoplasms. The "neoplastic" cell, in this case
a neoplastic THSC or PMSC. must have some form of relative growth
advantage as compared to the normal cells and secondly. its growth
must in turn somehow be suppressive for growth of the comparable
compartment of normal cells. Theoretically. these two characteristics
could be independent phenomenon or might be mediated by the same
mechanism. In any system which I've been able to envision which
would allow the neoplastic cell to take over the myeloid system,
there must be an abnormality in that cell with respect to its response
to normal, physiologic factors regulating the system. This abnormality
could range from complete autonomy of growth (a cell which would
continue to grow without regard to the presence or absence of physiologic
regulators) to subtle defects; such as. one in which the neoplastic
cell was simply more sensitive to growth stimulators or less sensi
tive to growth inhibitors than is the normal cell. In either event.
the normal v cells could become repressed by a variety of mechanisms.
As the neoplastic clone expanded the normal control system might
recognize the expanded neoplastic stem cell system and repress the
normal one or the neoplastic clone could even prod uce inhibitors
of the normal. Undoubtedly spurred on by the observation that most
megaloblastic anemias. once widely thought to be closely allied
to leukemia, were due to vitamin deficiency. along standing hypothesis
has been held by many that a least certain "leukemias" may represent
faulty regulatory systems rather than intrinsic neoplastic abnormality
of the cell identified as "leukemic". In my opinion. the demonstration
that these are clonal diseases, coupled with the demonstration that
the normal counterpart cells are either absent or repressed rules
out this hypothesis as a primary cause of the disease. There may
be abnormalities of the regulatory system as well. but I think these
must be con sidered secondary to the primary neoplastic process
rather than as playing a causative role. Just as the primary direct
evidence for clonality of disease comes from chromosome and isozyme
data, so does the evidence for the presence of some residual normal
stem cells. Is a chromosome abnormality an accurate marker as to
whether or not a cell is part of the clone of human leukemia? This
question cannot be answered with certainty. but there is growing
evidence, if of an inferential nature only, that it does not. I
think all would agree that all cells bearing the PhI abnormality
are part of the clone in CML and that cells bearing a consistent
chromosome abnormality in AML, PRY or IMF are part of that clone.
It is the converse situation where serious questions must be raised;
it is not clear that a cell not bearing the chromosome abnormality
is not part of the clone. A num ber of pieces of evidence suggest
that only a portion of the clone carries the chromosome abnormality.
Perhaps the strongest evidence suggesting that this is true are
the somewhat discrepant findings with respect to chromosome abnormalities
and isozyme studies in PRY and IMF [11,15]. The discrepancies may
be due to the fact that both studies have been done in a very limited
number ofpatients and parallel studies have not been done in the
same patient, but discrepancies are there none-the-less. All isozyme
studies to date in patients with active PRY and IMF have indicated
that all myeloid cells analyzed from the patients are part of the
clone. However. in those patients in whom a chromosome abnormality
has been found it often is present in only a portion of the analyzed
myeloid tissue [ 16]. Similarly. when a chromosome defect is present
in AML it often is not present in all analyzed myeloid tissue, even
when virtually 100% of the myeloid cells appears to be leukemic
on stained smears. This is also true for changes other than the
PhI in blastic crisis of CML [17] and quite discordant changes in
chromosome defects and morphology may be observed in blastic crisis
[ 18]. Although most patients with CML have the PhI chromosome in
all analvzed myeloid metaphases. some do not. The general assumption
is that the latter patients are chimeric, i.e. have persistence
of both normal and leukemic cells. an assumption which mayor may
not be true. When chromosome analvsis was carried out on granulocyte-macrophage
colonies grown in vitro, PhI negative colonies were found in some
patients in whom all direct metaphases had been positive [15]. This
suggested that normal stem cells were still present. but that they
were dormant in vivo. However, when Fialkow and coworkers (see Fialkow's
paper in this symposium) analyzed G-6 PD isozymes in individual
G-M colonies from patients with CML, no colonies were found which
were not part of the clone. Resulution of this seeming discrepancy
will require further studies in which both chromosomes and isozymes
are analyzed in colonies from the same patient. For the above reasons,
the use of the lack of chromosome markers to prove the persistence
of normal stem cells in these clonal diseases may be questioned.
Keeping that in mind, there is none-the less fairly strong evidence
that normal stem cells persist in these diseases but probably in
a quiescent state. First. and perhaps foremost, with respect to
the strength of the evidence is the development of remission in
AML. Suffice it to say that virtually all current evidence points
to remission in AML representing the re growth of the normal myeloid
system while the clone has been reduced and held in check by therapy.
Evidence is also quite strong for the persistence of normal PMSC
in PRY. All myeloid tissue taken directly from the patient for isozyme
analysis has apparently been part of the clone. However, when colonies
of erythroid tissue have been grown from the same patient, some
have been isozymically heterozygous (see Adamson's paper in this
symposium). This is compatible with the previously expressed concept
that the expanding neoplastic clone induces repression of normal
cells in vivo, but that they are still present. As noted above the
situation is not so clear in CML. In summary, there is strong evidence
that CML, AML, PRY and IMF are clonal diseases ofa pluriopotent
hematopoietic stem cell and suggestive evidence that PNH is such
a disease. There is strong evidence that CML is a disease of the
THSC and suggestive evidence that PRY may involve this cell; AML
more likely is a disease of the PMSC and IMF is a clonal disease
ofone of these two cells. The nature of the growth advantage enjoyed
by the abnormal cell as compared to the normal cell is unknown.
However, the data in hand strongly suggest that normal stem cells,
while still clearly present in some of the diseases, are quiescent
and not producing mature cells in most patients. Existing data appears
to rule out the possibility that any of these diseases is due to
faulty regulation by factors external to the stem cell itself.
References
I. Downey. H. (ed.): Handbook of Hematology. Vol. 3. p. 2025. New
York: IHafner Publishing 1938
2. Abramson. S.. Miller. R.G.. Phillips. R.A.: The identification
in adult bone marrow of pluripotent and restricted stem cells of
the myeloid and lymphoid systems. .1. Exp. Med. 145, 1567 (1977)
3. Millard. R. E.. Okell. S. F.: The effects of cystosine arabinoside
in vitro on agar colony forming cells and spleen colony forming
cells ofC-57BIL mouse bone marrow. Cell Tissue Kinet. 8,33 ( 1975)
4. Bennet. M.. Cudkowicz. G.. Foster. R. S. .Ir.. Metcalf D.: Hemopoietic
Progenitor cells of W anemic mice studied in vivo and in vitro.
j. Cell Physiol. 71,211 226 ( 1968)
5. Gregory. C..J.. Eaves. A.C.: Three stages of erythropoietic
progenitor cell differentiation distinguished by a number of physical
and biologic properties. Blood 51,527 (1978)
6. Williams. N.. jackson. H.. Sheridan. A. P. C.. Murphy. M.j.
jr.. Moore. M. A. S.: Regulation ofmegakaryopoiesis in long-term
murine bone marrow cultures. Blood 51,245 (1978)
7. Chervenick. P.A.. Boggs. D. R.: 1n vitro growth of granulocytic
and mononuclear cell colo nies from blood of normal individuals.
Blood 37,131 (1971)
8. Whang-Peng. .1.: Cytogenetic studies on acute myelocytic leukemia.
Blood 34,448 (1970)
9. Boggs. D. R.: Hematopoietic stem cell theory in relation to
possible lymphoblastic conver sion ofchronic myeloid leukemia. Blood
44,499 ( 1974)
10. Sandberg. A. A.. Hossfeld. 0. K.: Chromosomal abnormalities
in human neoplasia. Ann. Rev. Med. 21,379 (1970)
11. Fialkow. P.j.: Human myeloproliferative disorders: clonal origin
in pluripotent stem cells. Proc. 5th Cold Spring Harbor Symposium
(in press)
12. Fialkow. P.j.. Denmon. A.M.. jacobson. R.j.. Lowenthal. M.N.:
Chronic mvelocvtic leu kemia. Origin of some lymphocytes fr.om leukemic
stem cells. j. Clin. Invest. 62,815 ( 1978)
13. Wintr0bc. M.M.. Lee. R.E.. Boggs. O.R.. Bithe1. T.. Athens.
.I.W.. Foerster. j.: Clinical Hematology (7th edition). Philadelphia:
Lea and Febiger 1974
14. Hoffman. R.. Estren. S.. Kopel. S.. Marks. S. M.. McCaffrey.
R. P.: Lymphoblastic-like trans foormation of polycythemia vera.
Ann. Intern. Med. 89,71 ( 1978)
15. Chervenick. P. A.. E11is. L. D.. Pan. S. F.. Lawson. A. L.:
Human leukemic cells: In vitro growth of colonies containing the
Philadelphia (phI) chromosome. Science 174, 1134 (1971)
16. Whang-Peng. J.. Lee. E.. Knut.sen. T.. Chang. P.. Nienhuis.
A.: Cytogenetic studies in pa tients with myelofibrosis and myeloid
metaplasia. Leukemia Res. 2,41 (1978)
17. Srodes. C. H.. Hyde. E. F.. Pan. S. F.. Chervenick. P.A.. Boggs.
D. R.: Cytogenetic studies during remission of blastic crisis in
a patient with chronic myelocytic leukaemia. Scand. J. Haematol.
10, 130 ( 1973)
18. Gall. J.A.. Boggs. D.R.. Chervenick. P.A.. Pan. S.F.. Fleming.
R.B.: Discordant patterns of chromosomal changcs and myeloblast
proliferation during the terminal phase of chronic myeloid leukemia.
Blood 47,347 (1976)
|